
HealthNews
New info on the 11 diagnosed nurses

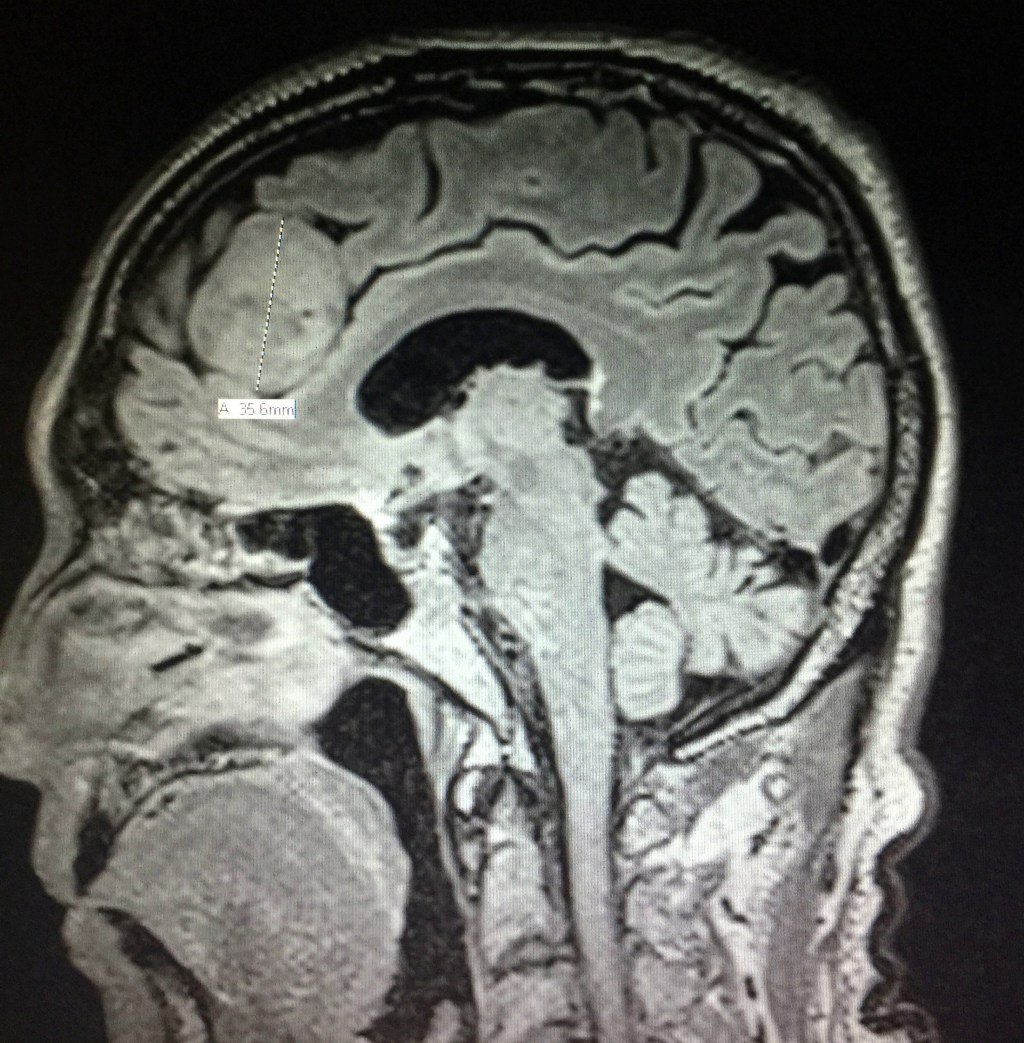
A new report on the investigation into a potential hospital cancer cluster is shedding light on the 11 nurses who were diagnosed with brain tumors.
Eleven current and former nurses in Newton-Wellesley Hospital’s fifth floor maternity wing were diagnosed with brain tumors, sparking concern from employees and the community.
Now, a new independent report of the tumor concerns at the hospital concluded that the hospital workplace is a safe environment — and is not the cause of the brain tumors. There’s no evidence of “a true workplace tumor cluster” at the Mass General Brigham facility, according to the Harvard professor’s report.
The external review provides some new information about the 11 diagnosed nurses, who are all women.
Six of the cases are meningiomas, two are gliomas, two are pituitary adenomas, and one is a schwannoma of the optic nerve. Except for the gliomas, the other nine tumors are all considered benign.
Here’s more information about the nurses:
Case 1: 50-59 years old; hired in 2000-2009; meningioma; imaging diagnosis
Case 2: 50-59 years old; hired in 2010-2019; meningioma; imaging diagnosis
Case 3: 30-39 years old; hired in 2010-2019; meningioma; tissue confirmed
Case 4: 50-59 years old; hired in 2010-2019; meningioma; possible imaging
Case 5: 50-59 years old; hired in 2010-2019; meningioma; tissue confirmed
Case 6: 50-59 years old; hired in 2020-present; meningioma; imaging diagnosis
Case 7: 50-59 years old; hired in 2000-2009; glioma; tissued confirmed
Case 8: 50-59 years old; hired in 2000-2009; glioblastoma; tissue confirmed
Case 9: 40-49 years old; hired in 2010-2019; pituitary adenoma; imaging diagnosis
Case 10: 20-29 years old; hired in 2020-present; pituitary microadenoma; imaging diagnosis
Case 11: 60-69 years old; hired in 1990-1999; optic nerve schwannoma; imaging diagnosis
HealthNews
I’m An ER Doctor. This 88-Year-Old’s Visit Left Me Stunned.


The computer said she was an 88-year-old female with a chief complaint of fatigue. From experience, I knew fatigue in an older person could be caused by almost anything. So … was it a heart attack? Depression? Cancer? An infection somewhere? Or was she just … fatigued?
The real reason she was there never crossed my mind.
The tiny woman had positioned herself precisely in the center of the gurney. Her white tennis shoes sat under the chair with a thick, flesh-colored knee-high stocking tucked inside each one. On the seat of the chair was a neatly folded yellow cardigan atop an equally neatly folded brown dress.
She wore her hospital gown like a jacket, open to the front, and her knobby hand clutched it closed over her cross-your-heart bra and waist-high white cotton panties. A Catholic cloth scapular with an image of the Virgin Mary hung on a string around her neck, and a tiny gold cross on a fine gold chain nestled in the hollow at the base of her neck.
Advertisement
“Hola. Mi nombre es Doctora Birnbaumer. Como se llama?” I said to her.
“Hola, Doctora. Mi nombre es Maria,” she replied.
Her eyes sparkled, and she sat up straighter, her posture that of someone who found life interesting. I checked her armband and offered to cover her with the sheet folded at her feet. She nodded.
I asked her how she was feeling. Fine, she told me. Was anything bothering her? No, she said. Any pain? No. Any shortness of breath, chest pain, headache? No, no and no. I went through my list and she denied anything being amiss.
Maria’s only encounters with the medical system had been for the births of her many children, several of whom she had outlived. She had been widowed over two decades before. She lived alone, with family nearby. She wasn’t working but had spent most of her life as a housekeeper. No meds, no allergies, no surgeries.
Advertisement
I asked if I could examine her, and she nodded. From head to toe, she was remarkably fit. Her bright, curious eyes nestled in a sea of soft skin and were bracketed by deep crow’s feet sculpted by years of smiling. The rest of her head and neck exam were normal. A tiny bit of curvature of the spine. Clear lungs, a strong, steady heartbeat with no abnormal sounds. Abdomen, extremities, neuro exam … all normal.
I was flummoxed. She watched me expectantly.
“So, are you sure nothing is bothering you today?” I asked.
She shrugged and raised her hands in a “what can you do?” gesture.
I was getting nowhere. Time for a different tactic.
I asked her why she was in the emergency room. She said she didn’t know.
Dead end.
New angle: “How did you get here today?”
Her face blossomed into a smile. Her daughter, granddaughter and great-grandson had come by her home, picked her up and brought her to the emergency department.
Finally. Maybe an answer.
With Maria’s permission, I sought out her family members in the waiting room. They were easy to find, all three resembling the petite woman on that gurney. The same dark eyes stared at me as I approached them, but while hers were bright and inquisitive, theirs were red-rimmed, and their eyelids were swollen.
Advertisement
As we entered the “family room” to talk, the two women deferred to the teenage boy, who acted as spokesman. He remained standing as the women and I sat.
They all turned to me, waiting. I cleared my throat.
“So, I was wondering, why did you bring Maria to the hospital today?”
Instantly all three sets of eyes filled with tears. The oldest woman nodded to the boy, and he spoke, dropping his gaze to the floor.
“My cousin. He died. The police came to my aunt’s house and told her he got shot.”
“Oh! I’m so sorry.” Now I understood the tears.
We sat for a few more moments in silence. No one moved. And I still didn’t know why Maria was there. I ventured, “So, is there something wrong with your great-grandmother?”
Advertisement
The boy answered. “My cousin. He is … was … Abuelita’s favorite. Everyone in the family knows it.” The boy’s voice was pleading, but I still didn’t understand. “We want you to tell her he’s dead,” he blurted.
And there it was.
I wish I could deny it, but my first reaction was irritation. Really? There was nothing medically wrong with her? The emergency room was packed with people, some were really sick, and I just spent 15 precious minutes on this? Did people really think the emergency room fixed everything?
Advertisement
Then the three of them started talking at once. They feared she’d have a heart attack or a stroke when she found out. They were terrified the news might kill her. They didn’t want to tell her. They wanted someone else to do it, and she needed to be somewhere that, if something terrible happened, she’d be taken care of.
I sat with what they told me for a moment. I recalled how I felt when my dad called me with the news that his thigh pain was from a tumor that had spread from a mass in his lung. I remembered how much I wanted someone to tell me it would be OK, that we would all survive this, that the world, now horrifyingly askew, would somehow right itself.
The healing that eventually happened didn’t result from any discussions with a doctor but grew from the love and support we gave each other as a family, from the times we would lean together, our hands and heads touching, creating an edifice, a steeple from which we could all draw strength.
Advertisement
Through these memories, my path forward became clear.
I took a breath and leaned forward to look each of them in the eyes. I made sure they heard me when I told them I was there for them, all of them … including Maria. I said I would be there with them, in the room, and around for hours to watch Maria if she needed anything and to make sure she was safe and taken care of. I told them I had their backs, but that the news needed to come from them.
They searched each other’s faces, and then they all nodded.
As we all walked into Maria’s room, her bright smile faded when she saw our faces. They moved to her bedside. I slid a box of tissues onto the table near Maria and stepped away.
Maria was now surrounded by the three generations of her progeny. They spoke to her in Spanish in hushed tones, and I watched as four lives — four generations — confronted the dreadful news.
Advertisement
Maria listened quietly. Her straight posture sagged the tiniest bit, her smile disappeared, and her face aged decades in moments. She reached one hand, spotted with age and deformed by years of labor, out to her family, and they all joined hands. With her other hand, she clutched her scapular, pulling gently on the string that attached it around her neck.
I eased out of the room, leaned against the wall in the hallway and remembered.
I remembered being a young woman deeply invested in caring for others and deciding my future was in medicine. I happily took on the years of schooling and training and debt required to become a doctor. I recalled the thrill of learning about the human body, how it works and what to do when it doesn’t.
I remembered cringing when I learned to start an IV and the patient gasped in pain. My heart broke the first time I told a patient they had a terminal disease. I cried myself to sleep the night when, as a third-year medical student, the man I assured would do fine during his coronary bypass surgery died on the operating table.
Advertisement
But I couldn’t remember exactly when my empathy started to slip away.
I knew that when I started my shifts, I walked through an ambulance bay packed with paramedics, gurneys and patients. I knew that no matter how hard or how fast I worked, the waiting room would never be empty. Patients came to the emergency department when they were injured and ill, but also when they could not get in to see their own physicians or when they lost their insurance or because after-hours was the only time they had off between jobs. Police brought in patients who had nowhere to go or had behavioral problems or whose addictions had consumed their lives.
There were never enough beds, patients waited for hours, and everyone — patients and staff alike — was understandably tired and angry. There was no way to do a good job — at least not as good a job as I had been trained to do. Despite that, administrative bean counters reduced my performance to counting how many patients I saw per hour and how many tests I ordered.
When I became an emergency physician, I had been all in on taking on the hard work and the erratic schedule, the difficult decisions and the busy shifts that went with the job. Over time, though, I had let the demands of a changing, overstressed and broken system knock me off course.
Advertisement
Standing in that hallway, listening to the soft murmurs of Maria and her family, I remembered why I was there — why I chose this profession, why I worked these crazy hours, why I did this job.
Maria didn’t have a heart attack or a stroke. An hour later, she sent her great-grandson to find me to tell me she wanted to leave. Her family helped her into her clothing and gathered her things as I prepared what was needed to send her home. At the door to her room, I hugged each of them in turn, Maria last, knowing her visit to the emergency room was exactly what she and her family needed.
Note: Some names and identifying details have been changed to protect the privacy of individuals mentioned in this essay.
Advertisement
Diane Birnbaumer is an emergency physician and writer living in Los Angeles. Her poems and essays have appeared in Intima: A Journal of Narrative Medicine and the medical journals Annals of Emergency Medicine and Annals of Internal Medicine, as well as the anthology “The Things They Wrote: A Writing/Healing Project,” published by Room: A Sketchbook for Analytic Action. She is an ambassador for The OpEd Project and attends The Writers’ Program at UCLA Extension.
This story was previously published on HuffPost and is being shared again as part of HuffPost Personal’s “Best Of” series.
Do you have a compelling personal story you’d like to see published on HuffPost? Find out what we’re looking for here and send us a pitch at pitch@huffpost.com.
HealthNews
World’s most infectious disease case found in California after they passed through super spreader hubs
A person infected with measles passed through San Francisco International Airport and two busy San Jose grocery stores, health officials have revealed.
The alert involves an adult from Santa Clara County who was infectious while passing through the major transport hub on Thursday morning between 8:30 a.m. and 11 a.m.
The individual moved through the international terminal, including passport control, customs and baggage claim areas.
Later that night, between 8 p.m. and 10 p.m., the same person visited two San Jose locations: Trader Joe’s and International Halal Market.
Anyone who was present at those sites during the specified time frames may have been exposed, officials said.
Because measles is among the most contagious diseases in the world, health authorities warned that symptoms could appear seven to 10 days after exposure and include fever, cough, runny nose, red eyes and rash.
Unvaccinated individuals are being urged to quarantine, avoid large gatherings and monitor for signs of illness for up to three weeks.
Officials also stressed that pregnant women, infants, immunocompromised individuals and the unvaccinated should seek medical guidance immediately if exposure is suspected.
Health officials warned that anyone developing symptoms should contact a medical provider before visiting in person, in order to reduce the risk of further transmission.
The situation comes as California records its highest annual measles count in seven years.
As of June 8, the state has confirmed 49 cases, already nearly double the total recorded in all of 2025 and the highest since 2019, when 73 cases were reported.
State data shows 94% of cases involve unvaccinated individuals, and more than 80% are in people under 19, highlighting ongoing gaps in immunity despite generally high vaccination coverage in the Bay Area.
Dr. Sarah Rudman, Santa Clara County’s health officer, emphasized that vaccination remains the strongest protection against measles and helps prevent widespread outbreaks even when exposures occur.
County officials are coordinating with the California Department of Public Health and the US Centers for Disease Control and Prevention on contact tracing tied to the exposure sites.
Santa Clara County has issued similar exposure warnings in recent years, including in February 2026 and May 2025, as measles continues to reappear in California through international travel cases and pockets of low vaccination.
Nationally, officials have also reported a broader resurgence, including a major outbreak in West Texas during 2025 that led to more than 750 cases, dozens of hospitalizations, and two deaths among unvaccinated patients.
Download The California Post App, follow us on social, and subscribe to our newsletters
HealthNews
Ebola one month on: will the latest outbreak in DRC become the most deadly yet?


When an orphanage in Bunia took in a newborn baby after his mother died from Ebola, the nuns who ran it hoped they were giving the infant a chance for life. The baby survived for only another two weeks. Now four of the nuns who cared for him have fallen sick with the deadly virus.
It is a snapshot of the tragedies at the centre of an outbreak in which the number of victims is roughly doubling every week, according to the World Health Organization (WHO).
“It’s really, really devastating,” says Dr Babou Rukengeza, Save the Children’s Ebola response lead in the Democratic Republic of the Congo (DRC). All the children and staff at the orphanage are now being monitored for symptoms.
A month on since the latest outbreak of Ebola, caused by the Bundibugyo virus, was first identified in the DRC, the latest figures from the UN show 676 confirmed cases and 136 deaths, the overwhelming majority in the DRC’s Ituri province.
Frontline workers say they are still battling shortages of the necessary supplies, including personal protective equipment and vehicles to transport dead bodies. Testing has improved, they say, but still needs to be done faster and carried out nearer to patients.
In neighbouring Uganda, which has reported 19 cases and two deaths, intensive tracing of contacts means the outbreak is under control, health officials say.
Despite the global risk remaining low, 22 countries, including the US, have imposed travel restrictions on people coming from the DRC, Uganda or South Sudan, according to Africa CDC, the health agency of the African Union.
Those restrictions have been criticised as impeding health agencies’ response. What the DRC really needs from the international community, experts say, is flexible funding that it can use to get the situation under control.
There are reasons for hope: scientists are working rapidly to test and produce vaccines against Bundibugyo, and the latest research suggests existing antivirals are likely to be helpful.
In Ituri, the organisations involved in the response meet daily to coordinate plans, and African leaders will meet virtually on Tuesday to discuss the outbreak and make funding commitments.
But there are also strong headwinds that are slowing the response: conflict continues in the worst-hit areas and misinformation is rife, leading people to avoid hospitals and the care that could save their lives, and there have even been attacks on aid workers and treatment centres.
Gratien Iracan, the local MP for the provincial capital, Bunia, noted on social media last week: “Despite the millions of dollars announced by the international community to support the response to Ebola, these resources are not yet sufficiently visible on the ground in Ituri.”
In subsequent posts, he highlighted a doctor’s death from Ebola, saying the medic had sent messages from his hospital bed complaining of poor care in the clinic. The Guardian has not been able to verify those messages.
Iracan also described an incident in which a community had called the authorities to report a suspected case of Ebola but the promised support had not arrived, sparking “incomprehension, anger and concern”.
According to Africa CDC, community trust is “a critical challenge” – CNN video footage from Bunia’s central market shows people denying the virus exists and blaming Red Cross workers for spreading it.
In a statement, the continental health watchdog cited “reports of resistance to hygiene measures and decontamination in some communities, as well as incidents of mob violence”.
A key reason for this stems from people’s reluctance to allow their sick relatives to be cared for by strangers in healthcare isolation units – and the importance of funeral rites.
For some people, their fear of displeasing God over not performing an appropriate burial for a relative can be greater than their fear of contracting a virus. According to one study after the 2016 outbreak, exposure to body fluids during each “unsafe” funeral for Ebola victims created an average of 2.58 secondary cases.
Informing people about the symptoms and risks – using mass media such as radio and TV as well as face-to-face contact in the community – has become a key part of work on the ground, says Rukengeza.
“We are pushing and currently we are working with the leaders, community leaders, religious and other people here on the ground just to let them know that this is really Ebola virus, and they have to pay attention,” he says.
With about 600 confirmed cases in one area, health experts would expect to have about 24,000 contacts to monitor. On Thursday, Dr Jean Kaseya, director general of Africa CDC, says there are 4,955 listed – and 57% of those are being monitored.
“It means there is a huge risk of transmission [being] sustained in the community,” Kaseya says. “We still have some confirmed cases not admitted [to hospital]. They are somewhere in the community, elsewhere.”
A joint response plan drawn up by Africa CDC and the WHO estimates that $518m (£387m) will be needed over the next six months to bring the outbreak under control. Kaseya says some early financial pledges from around the world “were not real”, but he now thinks that about $212m, including support in kind, was “almost there”.
Many of those infected are healthcare workers. Ebola is spread via body fluids, and those caring for the sick are most likely to be exposed to them.
Speaking from Bunia on Thursday, Dr Salim Abdool Karim, an epidemiologist who chairs the Africa CDC emergency consultative group, says he visited a treatment centre that day: “There were 22 patients in that particular hospital, five of whom were healthcare workers, two doctors and an anaesthetist.”
Even before Ebola arrived, Ituri faced a humanitarian crisis, with tens of thousands of people displaced by years of conflict. WHO officials have registered more than 520 security incidents affecting their teams in the field so far.
Over the past month, the outbreak has been gradually moving up the grim league tables that rank Ebola epidemics by case numbers and death toll. It is now the third largest on record. Modelling by the US Centers for Disease Control and Prevention suggests this outbreak could grow to match the 2014-16 one in west Africa, which killed more than 11,000 people.
“We hope we can stop that,” says Kaseya, “and it won’t move from the third to the second, even the first one.”
HealthNews
5 Exercises You Should Do In The Morning, According To Experts

There are no shortage of reasons why exercising regularly makes you feel good, no matter what time of day you choose to do it. However, if you have flexibility in your schedule, experts argue that an early workout can have positive and lasting effects on your entire day.
In addition to being “a great release for any tension your body holds,” said celebrity fitness expert Ridge Davis, “exercise helps build your endurance and ability to handle stress … the less stress you have, the more energy you have to use for your day.”
Advertisement
Since feeling mentally and physically exhausted aren’t at the top of anyone’s to-do list, it makes sense to get moving early.
“Being active has a profound impact on mental health by boosting and enhancing mental clarity and judgment,” added Magdalena Cadet, a board-certified rheumatologist at NYU Langone. “Exercise helps the body produce feel-good chemicals (endorphins) which can stimulate parts of the brain, help distract a person from anxiety as well as build confidence.”
Beyond boosting energy and reducing stress, morning exercise also benefits many of the body’s internal and external functions, like boosting metabolism, Cadet said. Consistent morning workouts can also enhance your sleeping habits.
Advertisement
“There are studies that suggest that early morning workouts may shift a person’s body clock so that there is more alertness in the early hours, which may result in improved sleep quality,” Cadet explained. The research showed that exercising at 7 a.m. may be the most optimal time.
Committing to a morning workout routine is an accomplishment on its own ― the best way to work out is to do something you enjoy. Fitness shouldn’t feel like punishment, but rather should be a celebration of movement and something you do to feel good. But, there are also specific moves you can do if you want to maximize the benefits of morning fitness. Here’s what experts suggest trying:
A full-body warmup
Advertisement
Before starting any morning exercises ― or if you just want to get some simple movement in ― certified personal trainer Lisa Mateo suggested doing some quick full-body work.
Mateo recommended stretching your “quads, hamstrings, hips, shoulders and triceps … along with a few cardio moves, like jumping jacks or high-knee runs, to get the heart rate going.”
A Tree Pose to activate your legs and core
Advertisement
According to Peloton yoga and meditation instructor Kristin McGee, the standing yoga posture known as Vrikshasana ― or Tree Pose ― is the perfect starting point for a morning exercise. The pose “promotes balance and stability in the legs and core,” McGee said.
McGee also credits the yoga move with “helping to focus the mind,” which is an important factor in “setting yourself up for a successful day.”
To properly execute Tree Pose, McGee instructs her students to “start by standing tall with your back straight, shoulders relaxed and both feet together (ankles and inner foot points touching).”
Advertisement
“Once feet feel firmly planted, shift your weight to your right foot, lift your left foot off the floor, bend your left knee and position your left foot onto the inside of your right thigh,” she continued.
Once your legs are in a stable position, your arms can remain in prayer position in front of your heart or you can raise them above your head. However, McGee advised anyone with concerns about their balance to “place your hand on the wall or a table for support or keep your foot lower at the ankle.” The pose should be held for five to 10 breaths and then repeated on the opposite side.
A Downward-Facing Dog to wake up your body and brain
Advertisement
Another great yoga move to do in the morning is Downward-Facing Dog. McGee is a fan of the pose because of its ability to “stretch and strengthen the entire body.” The move also “gets blood flowing to the brain, which is great for waking up,” McGee said.
The move, as its name suggests, is very much reminiscent of the way “a dog wakes up from a nap … and stretches their entire body with a nice arch,” McGee explained. Humans can mimic the motion by beginning on all fours keeping wrists in line with shoulders and toes tucked.
On an exhale, push your hips up and straighten your legs. Gently continue to push upward, engaging your arms while moving your shoulders away from your ears.
Advertisement
“Keep your core, legs and arms engaged and your kneecaps lifted, and pedal your legs back and forth to loosen up any tightness in the legs or lower back,” McGee added.
Dead Bug to fire up your core and prevent back pain
Davis said he personally loves doing a move called the Dead Bug in the morning to help with core stability. He relies on the exercise to “strengthen core muscles and prevent lower back injury,” he said.
Advertisement
This move is best performed on a padded mat, and proper form is vital to its success. To prepare for the move, Davis instructs clients to “lay on your back with knees bent and feet flat on the floor and arms straight alongside your torso.” Keep in mind that “the main goal is to keep the lower back firmly pressed into the floor during the movement,” he added.
Once in the starting position, lift your hands with elbows above your shoulders and fists facing each other. Exhale and raise your legs with knees directly over your hips then slowly lower your right arm and left leg until they’re just above the floor. (Here’s a video to give you more of a visual.) On an inhale, bring them back to the starting position and repeat the entire motion on the opposite side to complete one repetition. Beginners should aim for two to three sets composed of five reps on each side.
Squats to improve overall mobility
Advertisement
Cadet favors squats because they benefit many functions of the body all in one move.
“Squats are one of my favorite exercises, especially in the morning,” she said. “They help improve mobility while working the ligaments and connective tissue.” Squatting can also aid in joint support, she added.
However, beware if you have any injuries or conditions that may prevent you from doing this exercise.
“Individuals with knee, back or hip issues of any sort should avoid squats altogether or discuss modifications with a licensed professional,” Cadet said.
Advertisement
Correct form is the key to reaping rewards from squats. Begin with knees bent and feet flat on the floor. “Hips and ankles should be facing outward,” Cadet said, adding that you should not extend your knees past your toes and you should keep your legs no wider than shoulder width apart.
Envisioning your torso in a vertical line will straighten your posture and make the move more functional, Cadet said. Then, with your chest up and thighs parallel to the floor, tighten your abs and push your butt backward. Keep your core engaged while in position to help with stabilization.
HealthNews
2 daylight raccoon attacks within hours have New Jersey town eyeing rabies pellets
Ridgewood, New Jersey, is dealing with the fallout from two raccoon bites reported hours apart. The incidents sent a child and an adult for preventive rabies care and led officials to weigh an uncommon tactic: distributing oral vaccine bait for wild animals.
What happened?
WABC reported that one victim was an adult bitten on private property, after a 7-year-old boy had been attacked around 7 p.m. the day before near Maple Field & Community Garden and bitten on the upper leg.
WABC said the cases were reported close together in time, fueling concern that a raccoon in the area could be sick or acting abnormally. Both people received rabies treatment as a precaution.
So far, Animal Control officers searching the area have not found evidence of the raccoon. Residents are being asked to contact the Ridgewood Police Department if they see an animal that appears sick, injured, or unusually aggressive.
Why does it matter?
Rabies is rare in humans in the United States, but once symptoms appear, it is almost always fatal. Any bite from a potentially infected wild animal is a serious public health concern, particularly in places where children and pets may be nearby.
The attacks also underscore how closely people and wildlife overlap in many suburban communities. Raccoons are highly adaptable and often linger near gardens, yards, pet food, trash, and other human-created food sources, increasing the chances of bold or risky encounters.
As neighborhoods continue to expand into wooded areas and animals learn to associate people with easy meals, these encounters can become more common. When wild animals lose their fear of humans, the risks rise on both sides — people can be hurt, and the animal may ultimately need to be trapped or euthanized.
What’s being done?
One option now under discussion in Ridgewood is placing rabies vaccination pellets in wooded areas where animals gather, WABC reported. The flavored bait is meant to be eaten by wildlife, and federal agencies have used it for years to help curb the spread of rabies.
Officials say federal agencies do not consider the pellets dangerous to other animals, making the approach a practical way to reduce risk without trying to remove every raccoon from the area.
If you spot an animal acting strangely, report it rather than confront it. Preventing contact is the safest move for people, pets, and wildlife alike, and small changes at home can help reduce the chances of future encounters.
In communities where backyards, parks, and wooded habitats exist side by side, even a routine outing can quickly become a public health concern.




US and Iran reach peace deal | BBC News
US President Donald Trump has confirmed reports, initially from Pakistan, that the US and Iran have reached a deal. "Ships...


Trump says deal with Iran agreed and lifts blockade of strait of Hormuz | BBC News
US President Donald Trump has confirmed that the US and Iran have reached a peace deal. He has said the...


Anti-G7 march draws thousands on sidelines of summit
Demonstrators gathered in Geneva, Switzerland, ahead of the nearby G7 summit to denounce global inequality and heavy …


Mass protest at Stanford University graduation as soon as Google CEO Sundar Pichai takes the stage
A large group of graduates walked out of Stanford University’s commencement ceremony Sunday moments after Google CEO Sundar Pichai began...


Y2K called and….tan lines are back? | Engagement Party
Y2K called and they're saying…tan lines are back? Watch Audie Cornish and Ari Shapiro (and speicla guest Elise Hu) break...


How Heidi Blake documented Andrew Tate's ‘Empire of Abuse’
Investigative reporter and New Yorker staff writer Heidi Blake speaks to Paula Newton about her reporting on the allegations of...

Stephen A. Smith: Trump gets ‘far more love’ from UFC world than any other sport
CNN's Kasie Hunt talks to ESPN and Sirius XM host Stephen A. Smith who contrasts President Donald Trump's embrace by...


I’m An ER Doctor. This 88-Year-Old’s Visit Left Me Stunned.
The computer said she was an 88-year-old female with a chief complaint of fatigue. From experience, I knew fatigue in...


Royal Marines Take Control Of Russian Shadow Fleet Tanker | BBC Newscast
Royal Marine Commandos have boarded a Russian shadow fleet oil tanker in the English Channel in the early hours of...


'Let's not blow it!' Trump says after Israel strikes Beirut | BBC News
Iran's chief negotiator says there's "no point" in continuing talks with the US after Israel launched a strike on Beirut....
-

 LifestyleNews1 week ago
LifestyleNews1 week ago120 minutes of strength training per week may help extend lifespan
-

 Politics3 days ago
Politics3 days agoWhat to know about the stabbing that set off fiery riots in Northern Ireland
-

 Business1 day ago
Business1 day agoHow much of Musk’s wealth comes from government help? Virtually all of it
-

 Video2 days ago
Video2 days agoDownload fans say what they love about the festival. #DownloadFestival #BBCNews
-

 HealthNews3 days ago
HealthNews3 days agoThe people of Okinawa, Japan only eat until they are about 80 percent full, then stop — and the practice has been linked in multiple peer-reviewed studies to lower rates of cardiovascular disease, slo
-

 Video2 days ago
Video2 days agoWhy SpaceX IPO isn't about space. #SpaceX #ElonMusk #BBCNews
-

 Food2 days ago
Food2 days agoPope Leo’s plane was grounded. Then the King of Spain stepped in to help
-

 TravelNews2 days ago
TravelNews2 days agoMy Paternal Instinct Should’ve Warned Me About Netflix’s Maternal Instinct