
HealthNews
Her Mom Asked Her to Take Custody of Her Three Nieces if Her Health Fails, But She Doesn’t Know How She Can Afford It


It is always heartbreaking when someone loses custody of their kids. Even though it is hard, the best thing for the kids is if they can be cared for by family members.
What would you do if your mother was caring for your sister’s kids after she lost custody, but then Mom got sick and asked you to take the kids in?
That is the situation that the woman in this story is in, but she doesn’t think she can afford three more kids. She offered to have her mother move closer to her with the kids so she could help out, but Mom is unwilling.
This is honestly a very difficult situation, but in the end, I think she has to do what is best for her immediate family. Read through the full story below and see what you think she should do.
AITAH I don’t want custody of my sister’s 3 kids?
I (29F) have 1 kid (11F). My sister (32F) has 3 kids (11F, 8F, 6F). The oldest is also autistic.
What a sad situation.
About 3 years ago my sister lost custody of her kids. The girls were split up in the system for a little over a year before our mom (52F) got custody 2 years ago.
Over the last 2 years the girls have been really thriving. They’re happy, healthy, doing well in school…
Absolutely heartbreaking.
Recently my mom got some unexpected health issues that are severely impacting her mobility and energy. There is no cure. She called me last week to ask if I would take the girls so they aren’t split up in the system again. My heart sank.
I LOVE my nieces. There’s no denying that. And my daughter loves her cousins. The kids all get along great.
She clearly wants what is best for these young ladies.
They live on the opposite side of the country, but I visit whenever possible. I’m always planning all sorts of activities and experiences for them, and encouraging them to pursue the things they love.
The oldest loves art, the middle child loves gymnastics, and the youngest loves pokemon and video games. I plan things we can all do together and I make sure they each get one on one time too. I would die for these girls.
You can’t just pretend that taking custody won’t cost money.
But I just don’t have the means to care for them full time.
My husband and I are considered a low income family. After a decade of saving, we finally bought a small 2 bed townhouse, but there’s barely enough room for the 3 of us, let alone another 3 kids too.
The kids will have to move either way.
I suggested my mom move closer so I can help more day to day, but she shot that down rather quickly.
Her reasons were she didn’t want to pull the kids out of their current school (but I guess it’s ok if I do??), and with her health issues she didn’t want to have to find a new Dr (that one is pretty valid, there’s a serious health care crisis in my country).
They are offering some very reasonable options.
Us moving closer to them is not an option, we would both have to find new jobs and my husband’s current job has really good benefits we can’t afford to lose.
My mom is retired so the only thing tying her to her current location is her Dr.
She has to really think this through.
My heart is breaking. I don’t want to lose my nieces to the system again. I love the relationship we have.
But I don’t see how I could sustainably take on the 3 of them full time.
It really isn’t fair to be upset with her about the situation. What did the sister do to lose custody?
My mom and my sister have been calling me heartless and that I haven’t fully thought it through, but I have.
I’ve been thinking about it every day for over 3 years when my sister first lost custody.
This is undoubtedly a very difficult situation, but she has to do what is in the best interests of his own family. She has offered some good options, but Mom and his sister seem unwilling.
If you enjoyed this story, check out this post about a bus driver who is sick and tired of covering everyone else’s weekend shifts.
Let’s see what the people in the comments have to say about the situation and what should be done.
This really is a heartbreaking situation.
You can’t make decisions based on guilt.
Here is someone who works in the child protection field.
I agree with this commenter.
Her sister has no say in what happens.
No matter how badly she wants to help, she is not in a position to do so. This family needs to come together to figure out what is best for the kids. Thinking outside the box and coming up with potential solutions.
No matter what they choose, it isn’t going to be easy. Hopefully, they can figure something out. Even if the kids need to go to the foster system, the family can still see them.
HealthNews
Millions of Women Are Left Out of Menopause’s Moment


Cybele Maylone, 46, has been hearing about hormone therapy nonstop. Whether it is her friends going through menopause or posts from influencers on her social media feed, the subject has seemed unavoidable: who was on it, which doctor finally took their symptoms seriously and, most importantly, how good it felt to be on the medication. The hot flashes waning. Brain fog lifting. Sleep returning.
To Ms. Maylone, it sounds like a miracle drug. But for her and millions of other women, it is not an option.
She was diagnosed in 2023 with a type of breast cancer fed by estrogen, and now takes a drug that suppresses the hormone to reduce her risk of recurrence. While breast cancer is the most widely recognized reason women may not be able take hormone therapy, which delivers estrogen or progesterone through pills and patches, the list also includes endometrial cancer, certain cardiovascular issues, severe liver disease and blood clotting disorders.
Ms. Maylone and other women said they feel deeply frustrated that they can’t take a drug that so many women around them seem to have benefited from.
“The messaging about HRT is so positive and all-consuming right now,” Ms. Maylone said. It seems like “you can experience this phase of your life totally differently, and there is relief,” she added.
“I feel totally cut off from that,” she said.
Rebecca Hastings, 46, cannot take hormone replacement therapy because it raises the risk of blood clots, which she is already more likely to develop because of a genetic mutation that she carries.
Thank you for your patience while we verify access. If you are in Reader mode please exit and log into your Times account, or subscribe for all of The Times.
Thank you for your patience while we verify access.
Already a subscriber? Log in.
Want all of The Times? Subscribe.
HealthNews
Inside the ebola epicenter in Eastern Congo : NPR

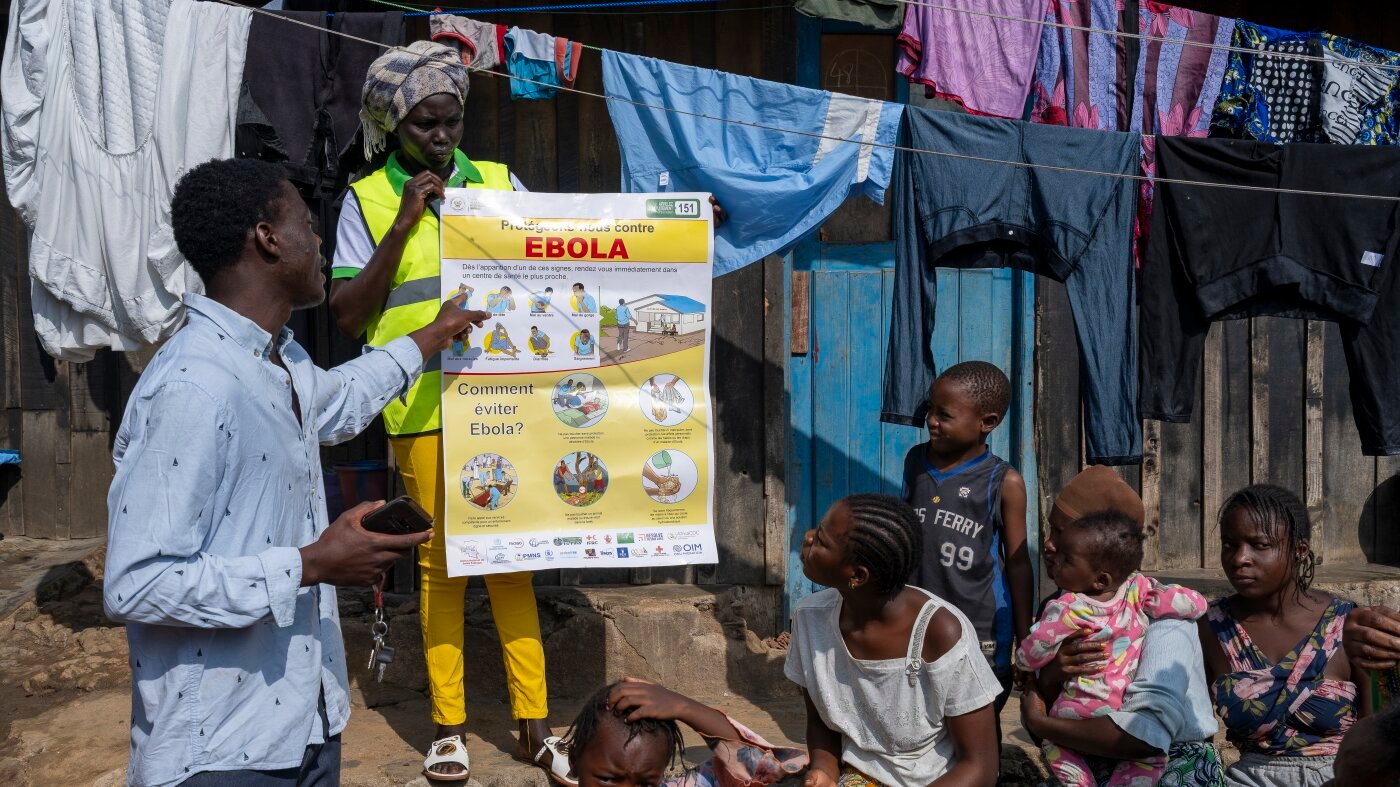
BUNIA, Democratic Republic of Congo — Eliezer Kasongo thought the Ebola epidemic would blow over in a few weeks.
Then the crisis began to unfold before his eyes.
“We started to see people die in the neighbourhood and we began to understand,” said Kasongo, a community volunteer in Bunia, the capital of Ituri province, in eastern Democratic Republic of Congo.
Despite once being a doubter, the 25-year-old now spends his days going door to door to try to raise awareness about the disease.
Ituri is the epicenter of Congo’s Ebola outbreak, which the government declared officially on May 15. The virus had likely been circulating for weeks before then, with cases clustered in a remote mining town called Mongbwalu.
Official figures show there are now 782 confirmed Ebola cases in eastern Congo as of June 13, and 181 confirmed deaths. Those numbers are an underestimate, according to health and aid officials, who point to testing delays as well as unnoticed deaths in villages and far-flung suburbs.
One month on from the outbreak’s announcement, signs of the Ebola response are everywhere in Bunia. Handwashing stations are ubiquitous and the central square blares announcements telling the people of Ituri not to panic.
A city of over 1 million people, Bunia now has the single largest number of cases — 212 — according to the official figures. Many residents are receptive to advice, according to Kasongo, but he and other volunteers sometimes meet resistance.
“There’s fear,” says Kasongo, “people are dying every day.”
On the day we arrived in the city, a sick man on a motorbike taxi vomited blood on his driver in the center of the city, and then died on the spot. Specialist teams came to retrieve the body and decontaminate the roadside, while his family members stood around and wept.
The driver fled the scene, according to witnesses. The incident underscores the difficulties health workers face in tracking down suspected cases — one of the most critical steps in stopping the spread of the disease.
Only 56% of contacts have been traced so far across the three Congolese provinces with active Ebola transmission, according to the Congolese health ministry. The task is particularly difficult in an environment where armed groups operate, roads are mostly unpaved, and towns and cities are densely populated.
The Democratic Republic of the Congo, despite its vast reserves of copper and cobalt, remains one of the world’s poorest countries. According to the World Bank, more than 85% of the population survives on about $3 a day.
Ituri, like much of eastern Congo, has also been devastated by decades of armed conflict. Its health system is severely underfunded. It is now coming under even more severe strain.
In a Bunia hospital called Clinique Universelle, a decontamination team spent the weekend scrubbing walls with chlorine solution. Several days prior, a patient at the hospital had tested positive for Ebola. The hospital then shut down.
The hospital director, Patient Mazirane, said that he and his colleagues had been working without personal protective equipment (PPE). Aid organizations have airlifted hundreds of metric tons of medicines and PPE to Ituri, but it’s still not enough. Many items, such as protective gloves, have to be changed regularly.
Dr. Mazirane, 38, said he wanted to leave the medical profession: if he dies, no one will look after his children. He says that several medical workers had already died.
“We’re not afraid, we’re very afraid,” he said.
HealthNews
Ebola cases in eastern Congo climb to 782 and deaths reach 181
KINSHASA, Congo (AP) — The number of confirmed Ebola cases in Congo has increased to 782, with 181 deaths, the Congolese Ministry of Health said in a statement on social platform X on Sunday evening.
However, the number of cases in Congo is believed to be higher because the outbreak was confirmed on May 15, weeks after it is suspected to have begun, and the contact tracing coverage rate is at 56%, a sharp decrease from last week.
The latest Ebola outbreak is caused by the rare Bundibugyo virus, which has no approved vaccine or treatment, unlike the “Zaire virus,” which was responsible for most of Congo’s past 16 outbreaks of the disease.
Fifty-six people have recovered, and the current fatality rate of the outbreak is 23%, the Ministry said.
The outbreak is concentrated in Congo’s eastern province of Ituri, which accounts for more than 90% of the cases. Cases have also been recorded in the North Kivu and South Kivu provinces, and have spread across the border to Uganda.
Nearly a million people have been displaced by conflict in Ituri, according to the U.N. humanitarian office, making contact tracing difficult as people flee attacks or move frequently in the vast province with dense forests, poor roads and remote villages that can take days to reach.
Tracing is also difficult among the thousands of artisanal miners who regularly move between remote sites in the mineral-rich region.
Attacks on health workers from angry residents, skepticism among some locals, and armed conflict in hot spots continue to challenge efforts to stop the outbreak.
HealthNews
Behind the Scenes at World Cup, Lots of Disease Busters


While millions of soccer fans cheer on World Cup matches in North America, health officials will be on high alert for germs. A heat wave may be the most obvious health threat, but infectious diseases can spread in a crowd, and experts are set to scrutinize wastewater, hospital visits, even social media for signs an outbreak may be afoot, per the AP. Measles, one of the most contagious diseases, is among the top concerns, sparking a warning this week from the Pan American Health Organization. With a nearly six-week stretch of packed stadiums, bars, and tourist sites in 16 cities, officials are on the lookout for a long list of infections, from the norovirus stomach bug to mosquito-borne dengue fever.
“This is truly a marathon,” says Palak Raval-Nelson, Philadelphia’s health commissioner. The mass gatherings come at a tense moment for budget-strapped health agencies in the US. The CDC, hit hard by Trump administration staffing cuts, already was grappling with a growing Ebola outbreak in Central Africa and a cruise ship hantavirus outbreak. While CDC officials have advised state and local health departments behind the scenes, its expected World Cup disease surveillance dashboard still was “in final development” days before the games began, per the Department of Health and Human Services.
“Our public health professionals are pretty stretched,” says global health specialist Rebecca Katz, who’s leading an unusual new hub to help. At the Health Security Operations Center, a joint effort between Georgetown University and MedStar Health, workers are analyzing data from around the country so they can alert health authorities, even ERs, to any early signs of trouble. The center is issuing daily “situation reports” on disease trends in host cities and team base camps to local and federal public-health groups, hospital officials, and others who’ve signed up.
People with certain viral or bacterial infections shed genetic material that sophisticated testing of wastewater can spot—an early warning system. For example, measles can appear in wastewater days before an ER sees initial patients. This week’s surveillance reports from Katz’s center note wastewater testing recently found rotavirus, hepatitis A, and norovirus in some parts of the US. In Dallas, a team is also enhancing mosquito testing, checking not just for West Nile virus that regularly spreads, but for viruses more common in other nations, like dengue and chikungunya. “It’s important that we don’t become alarmist,” says MedStar’s Dr. Shane Kappler. “We’re trying to be the insurance policy.” More here.
Read These Next
Climbing digs into the controversy over a boy’s feat
A famed ‘restaurant problem’
Vigilante livestreams innocent man
Police chief arrested on 70
HealthNews
I’m An ER Doctor. This 88-Year-Old’s Visit Left Me Stunned.


The computer said she was an 88-year-old female with a chief complaint of fatigue. From experience, I knew fatigue in an older person could be caused by almost anything. So … was it a heart attack? Depression? Cancer? An infection somewhere? Or was she just … fatigued?
The real reason she was there never crossed my mind.
The tiny woman had positioned herself precisely in the center of the gurney. Her white tennis shoes sat under the chair with a thick, flesh-colored knee-high stocking tucked inside each one. On the seat of the chair was a neatly folded yellow cardigan atop an equally neatly folded brown dress.
She wore her hospital gown like a jacket, open to the front, and her knobby hand clutched it closed over her cross-your-heart bra and waist-high white cotton panties. A Catholic cloth scapular with an image of the Virgin Mary hung on a string around her neck, and a tiny gold cross on a fine gold chain nestled in the hollow at the base of her neck.
Advertisement
“Hola. Mi nombre es Doctora Birnbaumer. Como se llama?” I said to her.
“Hola, Doctora. Mi nombre es Maria,” she replied.
Her eyes sparkled, and she sat up straighter, her posture that of someone who found life interesting. I checked her armband and offered to cover her with the sheet folded at her feet. She nodded.
I asked her how she was feeling. Fine, she told me. Was anything bothering her? No, she said. Any pain? No. Any shortness of breath, chest pain, headache? No, no and no. I went through my list and she denied anything being amiss.
Maria’s only encounters with the medical system had been for the births of her many children, several of whom she had outlived. She had been widowed over two decades before. She lived alone, with family nearby. She wasn’t working but had spent most of her life as a housekeeper. No meds, no allergies, no surgeries.
Advertisement
I asked if I could examine her, and she nodded. From head to toe, she was remarkably fit. Her bright, curious eyes nestled in a sea of soft skin and were bracketed by deep crow’s feet sculpted by years of smiling. The rest of her head and neck exam were normal. A tiny bit of curvature of the spine. Clear lungs, a strong, steady heartbeat with no abnormal sounds. Abdomen, extremities, neuro exam … all normal.
I was flummoxed. She watched me expectantly.
“So, are you sure nothing is bothering you today?” I asked.
She shrugged and raised her hands in a “what can you do?” gesture.
I was getting nowhere. Time for a different tactic.
I asked her why she was in the emergency room. She said she didn’t know.
Dead end.
New angle: “How did you get here today?”
Her face blossomed into a smile. Her daughter, granddaughter and great-grandson had come by her home, picked her up and brought her to the emergency department.
Finally. Maybe an answer.
With Maria’s permission, I sought out her family members in the waiting room. They were easy to find, all three resembling the petite woman on that gurney. The same dark eyes stared at me as I approached them, but while hers were bright and inquisitive, theirs were red-rimmed, and their eyelids were swollen.
Advertisement
As we entered the “family room” to talk, the two women deferred to the teenage boy, who acted as spokesman. He remained standing as the women and I sat.
They all turned to me, waiting. I cleared my throat.
“So, I was wondering, why did you bring Maria to the hospital today?”
Instantly all three sets of eyes filled with tears. The oldest woman nodded to the boy, and he spoke, dropping his gaze to the floor.
“My cousin. He died. The police came to my aunt’s house and told her he got shot.”
“Oh! I’m so sorry.” Now I understood the tears.
We sat for a few more moments in silence. No one moved. And I still didn’t know why Maria was there. I ventured, “So, is there something wrong with your great-grandmother?”
Advertisement
The boy answered. “My cousin. He is … was … Abuelita’s favorite. Everyone in the family knows it.” The boy’s voice was pleading, but I still didn’t understand. “We want you to tell her he’s dead,” he blurted.
And there it was.
I wish I could deny it, but my first reaction was irritation. Really? There was nothing medically wrong with her? The emergency room was packed with people, some were really sick, and I just spent 15 precious minutes on this? Did people really think the emergency room fixed everything?
Advertisement
Then the three of them started talking at once. They feared she’d have a heart attack or a stroke when she found out. They were terrified the news might kill her. They didn’t want to tell her. They wanted someone else to do it, and she needed to be somewhere that, if something terrible happened, she’d be taken care of.
I sat with what they told me for a moment. I recalled how I felt when my dad called me with the news that his thigh pain was from a tumor that had spread from a mass in his lung. I remembered how much I wanted someone to tell me it would be OK, that we would all survive this, that the world, now horrifyingly askew, would somehow right itself.
The healing that eventually happened didn’t result from any discussions with a doctor but grew from the love and support we gave each other as a family, from the times we would lean together, our hands and heads touching, creating an edifice, a steeple from which we could all draw strength.
Advertisement
Through these memories, my path forward became clear.
I took a breath and leaned forward to look each of them in the eyes. I made sure they heard me when I told them I was there for them, all of them … including Maria. I said I would be there with them, in the room, and around for hours to watch Maria if she needed anything and to make sure she was safe and taken care of. I told them I had their backs, but that the news needed to come from them.
They searched each other’s faces, and then they all nodded.
As we all walked into Maria’s room, her bright smile faded when she saw our faces. They moved to her bedside. I slid a box of tissues onto the table near Maria and stepped away.
Maria was now surrounded by the three generations of her progeny. They spoke to her in Spanish in hushed tones, and I watched as four lives — four generations — confronted the dreadful news.
Advertisement
Maria listened quietly. Her straight posture sagged the tiniest bit, her smile disappeared, and her face aged decades in moments. She reached one hand, spotted with age and deformed by years of labor, out to her family, and they all joined hands. With her other hand, she clutched her scapular, pulling gently on the string that attached it around her neck.
I eased out of the room, leaned against the wall in the hallway and remembered.
I remembered being a young woman deeply invested in caring for others and deciding my future was in medicine. I happily took on the years of schooling and training and debt required to become a doctor. I recalled the thrill of learning about the human body, how it works and what to do when it doesn’t.
I remembered cringing when I learned to start an IV and the patient gasped in pain. My heart broke the first time I told a patient they had a terminal disease. I cried myself to sleep the night when, as a third-year medical student, the man I assured would do fine during his coronary bypass surgery died on the operating table.
Advertisement
But I couldn’t remember exactly when my empathy started to slip away.
I knew that when I started my shifts, I walked through an ambulance bay packed with paramedics, gurneys and patients. I knew that no matter how hard or how fast I worked, the waiting room would never be empty. Patients came to the emergency department when they were injured and ill, but also when they could not get in to see their own physicians or when they lost their insurance or because after-hours was the only time they had off between jobs. Police brought in patients who had nowhere to go or had behavioral problems or whose addictions had consumed their lives.
There were never enough beds, patients waited for hours, and everyone — patients and staff alike — was understandably tired and angry. There was no way to do a good job — at least not as good a job as I had been trained to do. Despite that, administrative bean counters reduced my performance to counting how many patients I saw per hour and how many tests I ordered.
When I became an emergency physician, I had been all in on taking on the hard work and the erratic schedule, the difficult decisions and the busy shifts that went with the job. Over time, though, I had let the demands of a changing, overstressed and broken system knock me off course.
Advertisement
Standing in that hallway, listening to the soft murmurs of Maria and her family, I remembered why I was there — why I chose this profession, why I worked these crazy hours, why I did this job.
Maria didn’t have a heart attack or a stroke. An hour later, she sent her great-grandson to find me to tell me she wanted to leave. Her family helped her into her clothing and gathered her things as I prepared what was needed to send her home. At the door to her room, I hugged each of them in turn, Maria last, knowing her visit to the emergency room was exactly what she and her family needed.
Note: Some names and identifying details have been changed to protect the privacy of individuals mentioned in this essay.
Advertisement
Diane Birnbaumer is an emergency physician and writer living in Los Angeles. Her poems and essays have appeared in Intima: A Journal of Narrative Medicine and the medical journals Annals of Emergency Medicine and Annals of Internal Medicine, as well as the anthology “The Things They Wrote: A Writing/Healing Project,” published by Room: A Sketchbook for Analytic Action. She is an ambassador for The OpEd Project and attends The Writers’ Program at UCLA Extension.
This story was previously published on HuffPost and is being shared again as part of HuffPost Personal’s “Best Of” series.
Do you have a compelling personal story you’d like to see published on HuffPost? Find out what we’re looking for here and send us a pitch at pitch@huffpost.com.




Mariska Hargitay calls Jamie Lee Curtis a ‘family member’ | Variety & CNN Actors on Actors
Mariska Hargitay and Jamie Lee Curtis bond over their friendship in this behind-the-scenes of their Actors on Actors episode.


Teenagers react to the social media ban announced in the UK. #BBCNews


Parents react as PM Keir Starmer announces ban on social media for under-16s | BBC News
Keir Starmer says under-16s will be banned from social media by spring 2027. "A full ban is the right choice…...


What do we know so far about theUK social media ban?


Jamie Lee Curtis and Mariska Hargitay argue over pronunciation of Los Angeles
Whose side are you on? Stream the full episode now on the CNN app. Jamie Lee Curtis and Mariska Hargitay...


PM says UK will work to ensure 'lasting peace' after US-Iran deal. #BBCNews


Iran deal: Ex-NATO commander reveals ‘the bad news’
The US and Iran say they have reached an agreement that will end a US blockade of Iranian ports and...


Two men found guilty over arson attacks linked to UK PM Keir Starmer | BBC News
Two men have been found guilty of conspiring to carry out arson attacks on property and a car connected to...


Will prices come down after Iran and US agree deal to end war? #Iran #US #BBCNews


Camel milk is big money for rural China
China and Mongolia hold some of the world's largest populations of Bactrian camels, and their increasingly popular milk has …
-

 LifestyleNews2 weeks ago
LifestyleNews2 weeks ago120 minutes of strength training per week may help extend lifespan
-

 Business2 days ago
Business2 days agoHow much of Musk’s wealth comes from government help? Virtually all of it
-

 Politics4 days ago
Politics4 days agoWhat to know about the stabbing that set off fiery riots in Northern Ireland
-

 Video3 days ago
Video3 days agoDownload fans say what they love about the festival. #DownloadFestival #BBCNews
-

 Video3 days ago
Video3 days agoWhy SpaceX IPO isn't about space. #SpaceX #ElonMusk #BBCNews
-

 HealthNews3 days ago
HealthNews3 days agoThe people of Okinawa, Japan only eat until they are about 80 percent full, then stop — and the practice has been linked in multiple peer-reviewed studies to lower rates of cardiovascular disease, slo
-

 TravelNews3 days ago
TravelNews3 days agoMy Paternal Instinct Should’ve Warned Me About Netflix’s Maternal Instinct
-

 Food2 days ago
Food2 days agoPope Leo’s plane was grounded. Then the King of Spain stepped in to help