
HealthNews
Flu outbreak among Air Force recruits at Joint Base San Antonio after Hegseth ends mandatory flu vaccine


The basic training facility for the Air Force in San Antonio, Texas, is experiencing a flu outbreak following the end of mandatory vaccination for all service members.
As of Wednesday, there are at least 159 known cases among recruits and two hospitalizations at Joint Base San Antonio, two sources familiar with the matter told ABC News. One source told ABC News the number of cases and hospitalizations may be higher.
The outbreak comes after Defense Secretary Pete Hegseth announced in April that the annual flu vaccine would be optional for all U.S. military personnel, both active and reserve.
Previously, the flu vaccine was mandatory, but the new policy is in line with a previous change of making the COVID-19 vaccine optional.
The Pentagon has granted the military services exceptions to the policy, so the flu vaccine can be required in certain cases.
An Air Force spokesperson confirmed the outbreak to ABC News and said in a statement that over the last three weeks there has been a “localized influenza outbreak among trainees at Basic Military Training.”
“Medical professionals and Public Health officials have implemented mitigation measures to isolate and treat symptomatic trainees to reduce further exposure and continue to monitor the situation,” the statement read. “Medical personnel are also monitoring trainees who were in close contact with sick members in case they become symptomatic.”
The spokesperson said symptomatic trainees are receiving “the appropriate care” including antiviral medications such as Tamiflu.
“Once they are cleared by medical professionals they will return to training,” the statement said.
Earlier this year, when Hegseth ended mandatory vaccination, he referred to the policy as “overly broad and not rational.”
“Our new policy is simple: If you, an American warrior entrusted to defend this nation, believe that the flu vaccine is in your best interest, then you are free to take it; you should. But we will not force you,” Hegseth said.
The sources told ABC News that there is 40% flu vaccination rate among recruits at the San Antonio base since the mandate was lifted. Previously, the rate was nearly 100%.
Chief Pentagon spokesman Sean Parnell told ABC News that the Defense Department recently granted exceptions to the policy for the Army, Navy, Air Force, National Security Agency (NSA) and Defense Health Agency (DHA) through the Under Secretary of Defense for Personnel and Readiness.
“The decisions were based upon thorough risk assessments and are designed to maximize operational readiness, lethality, and force generation, while safeguarding at-risk populations,” Parnell said. “The Army, Navy, Air Force, NSA, and DHA are responsible for implementing the [exceptions to the policy]. The Department remains committed to the health and readiness of our warfighters and civilian personnel.”
The annual flu vaccine is currently recommended to everyone over 6 months old between September and the start of November. Although the typical flu season ends by February or March, people can become infected at any time.
People who travel internationally or live in group settings are at higher risk of transmitting and acquiring infectious diseases.
Public health specialists have warned that military members may suffer unnecessary complications from the flu after the vaccination mandate was ended and fear that severe cases will continue to climb in subsequent flu seasons if preventive vaccinations aren’t given to those most at risk.
Evidence has shown that young recruits are much more vulnerable to severe infection from influenza compared to other service members, though lower than the general population due to the military having historically high immunization rates.
A study published last year by the Defense Health Agency found that from the 2010-2011 to the 2023-2024 flu seasons, the highest rate of influenza hospitalizations among active service members were among those under the age of 25, especially young recruits.
The flu vaccine has been required for the military since 1945, at the end of World War II, partly tied to the threat of biological warfare use by rival nations and as well as the devastation that the flu pandemic of 1918-1920 wreaked on U.S. troops, according to a 2022 analysis from Wright State University in Ohio and the U.S. Air Force.
It’s estimated that between 20% and 40% of Army and Navy personnel fell ill, with more than 26,000 deaths among U.S. soldiers during the 1918-1920 flu pandemic.
After researchers noticed the effectiveness of the vaccine fading, the mandate was withdrawn in 1949. This was later found to be caused by abrupt and major changes to the flu virus — and the mandate was reinstated in the early 1950s after the changes became “clearer and combatable,” according to the analysis.
HealthNews
Shingles vaccine(s) and dementia: the only medical intervention to work faster than Tums

I am going to talk about how fast shingles vaccines reverse dementia across 4 papers. Turns out the effect is near instant. But before I do that, let us agree on some facts about the nature of the evidence used to make these claims.
Fact: Observational studies and even “natural” experiments have methodologic challenges.
People who get a vaccine and those who don’t are different.
If you see a doctor, you are more likely to get a diagnosis. Show me a healthy person, and I will show you someone who hasn’t gotten enough tests.
Diagnoses change over time. A dementia diagnosis in 2017 and 2018 may not be the same thing. Doctors may become more or less disease aware. They may be incentives to add diagnoses to the chart to make more money. They may code the same exact forgetful elderly man differently* based on a single calendar date.
Doctors may consciously or unconsciously offer more preventive care to people who appear well.
The medical record aka “chart” doesn’t truly capture how well people look.
Here are some other facts, which I don’t think can be disputed
There has been no truly successful treatment for dementia. We have a few drugs with effects so abysmally poor, we can debate if they work at all. Dementia is not a disease with a series of advances. It seems like we barely understand it biologically.
This is despite huge financial investments.
Dementia is a slow process that takes years to manifest. By the time you forget who you are, you have likely had symptoms for a long time.
With this background, lets turn to a scientific hypothesis:
What if the shingles vaccine reduces dementia?
I am willing to consider this hypothesis. Maybe less episodes of shingles— which is debilitating— and you get less dementia. Probably would take a few years or maybe a decade to see the benefit, if true. Powering a randomized trial for this would be gargantuan. Observational studies or natural experiments are probably useless due to the challenges with the data and endpoint adjudication, but that never stops a scientist up for promotion.
Now let us look at the 4 papers:
“Experts” offer a series of papers making ludicrous claims. They argue because the claim is consistently ludicrous— it must be true— rather than the same sources of bias plague the literature. The earth is flat because it looks flat when you look around in every direction.
In annals of IM this week.
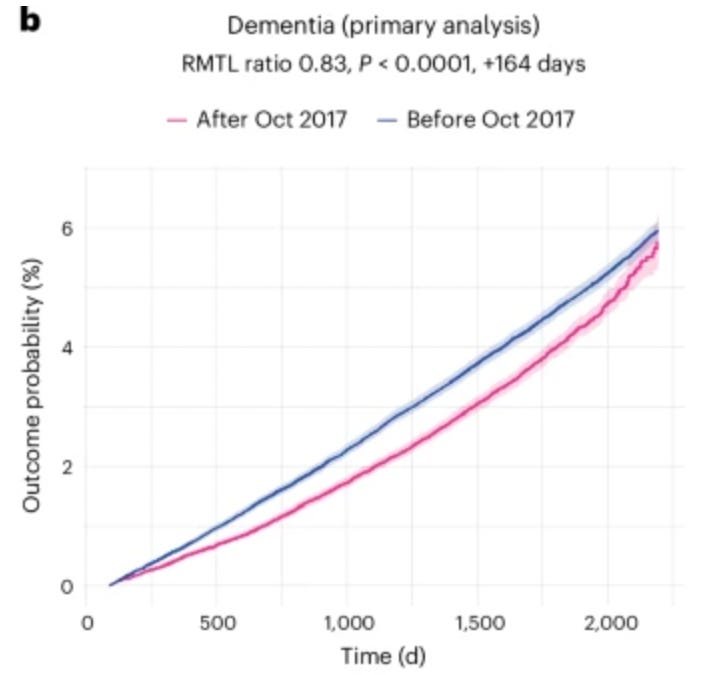
Wait, if you get ADMITTED to a nursing home—in less than a year—maybe as soon as 200 days—you get less dementia because of the Shingles vaccine. Within 3 years there is a 5% ABSOLUTE reduction in dementia. This vaccine must go inside neurons and repair them. It is what Ponce De Leon was looking for. A huge effect size that is also rapid.
In the JAMA paper, by 100 days, the shingles shot is already halting dementia. I don’t have dementia— at least I think I don’t— if I get 3 doses, I will probably be able to build Anthropic or Space X in a week— the brain benefit is so rapid.
The Wales paper doesn’t include K-M time to event plots. Sad. Why omit data when it will be so amazing? The US data is great. Obviously it confirms that the effect is near immediate.
And it includes a hazard function— thank you!— which makes it easier to see the fast action of the shingles vaccine. It makes Tums look slow acting.
Wait, what if this is true for every vaccine given to adults. What if the effect is not just shingles vaccines, but all vaccines. Perhaps they are miraculous as a class.
Check out this meta-analysis— it is true. Every vaccine prevents dementia!
Which is more likely?
Shingles vaccines (and maybe all sorts of other vaccines) instant act to reverse dementia. Even though nearly no drug in 50 years has achieved this. Despite tremendous effort and hundreds of billions of dollars. And this discovery just so happens to occur at a contentious time when vaccine science has taken on a left-right political bent, and coincidentally all the liberal outlets know the truth, while the conservative outlets spread misinformation (Option 1)…. or
The speed of the result is preposterously fast, the pretest probability abysmally low, and the desire to deceive ourselves astronomically high. (Option 2)
Future steps
Write to the annals of internal medicine and ask the editors to make the authors provide a Kaplan-Meier (time to event plot) of all cause mortality. (falsification endpoint)
Write to the Wales/ nature editors and ask for a time to event plot for dementia.
My understanding is that the NIH is planning on commissioning a randomized trial on this question. Encourage them to do so. (Equipoise is in the population of individuals who would do it, if and only if, this claim were true).
If there is a betting market on this trial, get a shingles shot to boost brain health before you vote.
Conclusion
The media coverage of this topic is deeply concerning. As I wrote recently in Sensible medicine, the media is unable to cover health and medicine without in house expertise in clinical trial appraisal. The status quo is untenable.
Coming soon, let me discuss that whole body ultrasound 😉
PS, if you enjoy these analyses, please subscribe
*say before or after a 2024 election
HealthNews
42 babies die in Australia as cases of devastating STI spike in US


Cases of a devastating STI are on the rise and newborns are at high risk for deadly complications.
The deadly and entirely preventable disease has claimed the lives of 42 babies in Australia, and a spike in cases in the US has experts worried about a potential uptick in domestic deaths.
Across the US, syphilis cases have risen sharply over the past decade. In states like New York, infections have increased fivefold since 2013, reflecting a broader nationwide trend.
Last month, several California counties reported particularly alarming rates.
Even more concerning, federal data shows congenital syphilis — when the infection is passed from a pregnant mother to her baby — has skyrocketed by 700% compared to roughly ten years ago.
“As a physician and former public health official, I have never been more concerned about those rates of congenital syphilis,” Jeffrey D. Klausner, a clinical professor of medicine at the Keck School of Medicine of the University of Southern California, wrote in an op-ed for STAT this week.
Left untreated, congenital syphilis can lead to miscarriage, premature birth, skeletal abnormalities, neurological problems, developmental delays, stillbirth or infant death shortly after birth.
In 2024, the CDC reported nearly 4,000 new cases of congenital syphilis, the highest case number since the mid-1950s.
In Australia, the disease has been the cause of 42 infant deaths in the past decade and a source of infection for countless others, leading the country’s Chief Medical Officer to deem it a “communicable disease incident of national significance.”
“It worries us a lot. It’s 100% important not to allow it to spread and to become endemic,” University of Adelaide Emeritus Professor Maciej Henneberg told the outlet.
Syphilis is spread by vaginal, anal or oral sex. Symptoms typically emerge 10 to 90 days after exposure, starting with a painless sore at the site where the bacterium Treponema pallidum enters the body.
The sore can heal on its own in three to six weeks, even as the infection persists.
In the next stage of infection, symptoms can include a rash, fever, fatigue, sore throat, swollen lymph nodes and hair loss.
If not addressed, it can devastate the brain, heart, and nervous system, leading to blindness, paralysis, and even death.
Syphilis is typically diagnosed with a blood test.
Despite progress in reducing other sexually transmitted infections like chlamydia and gonorrhea, congenital syphilis has continued to climb year after year in the US.
By 2024, it marked 12 consecutive years of increases, reaching its highest level since 1994.
According to the CDC, most cases of congenital syphilis are the result of pregnant women not being tested for syphilis or not being properly treated when they test positive.
Lack of insurance or access, fear of immigration detention, substance use and mental health problems can all create barriers to proper prenatal care and testing.
Even among women who do receive appropriate prenatal care, only 80% are tested for syphilis.
The disease can be effectively treated — and cured — with antibiotics such as penicillin, particularly when caught in its early stages.
“It is entirely preventable, so even if a pregnant person got syphilis, we can totally treat that pregnant person, and then the baby will not be at risk any longer,” Dr. Kelly Hosking, director of sexual health and blood-borne viruses strategy and policy for NT Health, told ABC News Australia.
In 2024, in response to rising syphilis rates, New York implemented a new requirement for syphilis screening.
Pregnant women must now be tested for syphilis at their first prenatal appointment, in their third trimester (between weeks 28 and 32), and at delivery.
Still, Klausner says there is more that can be done on a national scale to treat and prevent congenital syphilis, including making rapid point-of-care tests and same-day injectable penicillin treatment available in clinics and testing locations.
Klausner also underscored the importance of integrating prenatal care and substance abuse treatment to ensure high-risk populations have access to testing and treatment.
“Dead babies have no voice, and the families devastated by congenital syphilis are too stigmatized to speak up,” he said. “Physicians and those who care about children’s health must loudly advocate and demand attention from our public health leaders.”
HealthNews
Hunter-gatherers in Siberia died of a plague outbreak 5,500 years ago


Plague swept through groups of hunter-gatherers in southeastern Siberia 5,500 years ago, leaving dozens dead in its wake—with DNA from Yersinia pestis bacteria still trapped inside their teeth.
University of Oxford ancient DNA researcher Ruairidh Macleod and his colleagues recently sequenced the telltale bacterial DNA in teeth from plague victims at four ancient cemeteries in the area around Russia’s Lake Baikal. The tragedy that befell these communities is now the earliest known plague outbreak, courtesy of the oldest strain of Y. pestis ever sequenced.
Unearthing a new backstory for the plague
Until recently, scientists who study the evolution of diseases have held two fairly solid ideas about the origins of plague, the disease caused by Yersinia pestis bacteria. It’s a scourge so awful that it has gone down in history as not just a plague but the plague. The first idea is that the earliest strains didn’t have the right genetic traits to be really lethal. And the second is that the plague first began menacing humans when the first farmers settled in densely packed towns alongside rats and domestic animals.
But the dead of Ust’-Ida I cemetery, near Lake Baikal, tell a very different story.
“Our findings demonstrate that the earliest known outbreaks of plague occurred in prehistoric hunter-gatherers centuries before infections are observed in Neolithic farmers,” wrote Macleod and his colleagues in their recent paper.
That challenges our previous assumption that plague spillover was a side effect of people taking up farming and settling in permanent villages and towns, living closer to each other and to an assortment of animals (and their fleas).
“Much of the accepted theory around epidemiology of disease in the past is that this kind of thing shouldn’t occur in hunter-gatherers because hunter-gatherers are constantly moving around the landscape because they’re in such small groups all the time,” said Macleod in a press conference. “The theory, at least, is that infectious disease can’t really take hold and devastate entire communities in this way.”
So much for that theory.
Welcome to the world’s first plague cemetery
The Angara River flows from the depths of Lake Baikal. The people who lived along it thousands of years ago survived by hunting, foraging, and fishing. They would have lived in relatively small groups, but they seem to have stayed connected across hundreds of kilometers through marriage and family ties. Although their lifestyle would have been one of constant movement, they buried their dead in cemeteries such as Ust’-Ida, interring them with offerings of clay pots, stone tools, and bone and antler points.
At Ust’-Ida, archaeologists with the Baikal Archaeology Project unearthed a grim mystery: an unusually high number of dead children, a cluster of radiocarbon dates suggesting that many of the cemetery’s occupants died at around the same time, and no evidence of violence. Something tragic happened to this ancient hunter-gatherer community, but what? Archaeologists thought ancient DNA might shed some light on the mystery.
Macleod and his colleagues started with shotgun sequencing, a technique used to identify the DNA sequences in a sample when scientists don’t know exactly which organisms they’re looking for. They used samples from the roots of 46 ancient people’s teeth from four different cemeteries along the Angara River.
And to their complete surprise, they found plague.
Fun fact: Because dental roots are fed by lots of blood vessels, anything in your bloodstream is likely to pass through your teeth at some point, which means if you die with the plague, it may leave its DNA behind in your teeth. “This is really cool evidence that the plague was in the bloodstream, which is lethal,” said co-author Frederik Seersholm, a University of Copenhagen ancient DNA researcher who clearly knows a fun fact when he sees one, in a press conference.
About 11 of the 31 people Macleod and his colleagues tested at Ust’-Ida had Y. pestis DNA in their teeth, and Macleod says that’s “consistent with pretty much everybody [in the cemetery] having died of plague,” not just those 11. That’s because the detection rate for plague DNA in the remains at Ust’-Ida matches that at Smithfield’s, a known mass grave specifically for plague victims in London. It’s safe to assume everyone buried there had the plague.
“We really didn’t know what to expect going into this, so it was a complete surprise that we discovered this really, really early evidence for large-scale lethal outbreaks of plague amongst these hunter-gatherer communities at this point in time,” said Macleod in the press conference.
Ancient DNA and future outbreaks
Macleod and his colleagues managed to sequence a full Yersinia pestis genome from at least one of the samples, and it turns out to be the oldest strain of Y. pestis ever sequenced. According to the research, it’s very close to the base of the plague family tree, emerging just a few hundred years after Y. pestis last shared a common ancestor with another bacterium called Yersinia pseudotuberculosis. This ancient plague isn’t quite the one we’re familiar with today or the version that devastated medieval Europe.
This very early version of Yersinia pestis doesn’t have some of the genes that made its descendants so virulent; it’s missing, for example, a gene that produces Yersinia murine toxin, which helps the bacteria survive passing through a flea’s digestive tract on its way from a wild prairie dog to an unlucky hiker. It also lacks the right genes to form buboes (the painful swelling and darkening of the lymph nodes that gives bubonic plague its name). But its genome, not to mention the bodies it left in its wake, reveals that this early strain of Y. pestis was still horrifically deadly and probably deeply unpleasant to have.
“There are really a kind of perfect cocktail of other types of virulence genes that cause it to be so deadly—particularly, unfortunately, for children,” said University of Copenhagen evolutionary geneticist Eske Willerslev during the press conference.
Understanding that perfect cocktail could be useful for battling modern epidemics, despite this strain of Y. pestis being so different from the ones circulating now in North America and Asia.
“What it gives you is an idea of which mutations in combination {…} are something that survives in nature,” said Willerslev. Because any combinations of features that work well tend to reappear (in the same microbe or in a different species), he said, studying ancient bacterial DNA “actually gives you some information on how these pathogens, including the plague, will develop.”
Why did the plague kill so many children?
Bubonic plague spreads through flea bites, but pneumonic plague is a respiratory disease, which spreads in a similar way to the flu or COVID-19, and that seems to be how this early version would have passed from person to person. So we can assume it would have come with respiratory symptoms like cough and difficulty breathing, along with fever. But for children, it probably would have been even worse.
When archaeologists plotted the ages of the dead on a graph, they noticed a sharp peak in children between 7 and 11 years old. Adults older than 20, on the other hand, had the lowest death rate. That lines up with data from plague outbreaks thousands of years later in London, when parish records document local children bearing the brunt of the plague’s death toll.
The Y. pestis genomes that Macleod and his colleagues sequenced offer a clue about why. According to Iversen, the 5,500-year-old strain carries a gene that makes what’s called a superantigenic toxin: a chemical that triggers a dramatic, disorganized overreaction by the immune system. Children are especially vulnerable to this kind of reaction, said Oxford University immunologist Astrid Iversen during the press conference, because their immune systems are still learning how to respond to pathogens.
Telling the story of an ancient outbreak
The outbreak probably started when the bacteria made the leap from an infected marmot (a type of ground squirrel that’s still a common plague carrier in the area) to a single person and then spread like wildfire through several interconnected hunter-gatherer groups along the river. For millennia, people around Lake Baikal have hunted marmots for food and for their fur, and close contact with a plague-ridden marmot can spread the infection. This is how it goes: accidentally inhale a few droplets of blood while skinning your latest kill or eat an undercooked marmot stew, and you’ve just doomed your whole band. And the neighbors.
That scenario is supported by the fact that people at Ust’-Ida carried the same strain of plague as those buried 37 kilometers away at another cemetery, Shumilikha, which is what epidemiologists would expect to see if they were part of the same outbreak. The burial customs at the two cemeteries suggest they belonged to different subcultures within the wider Isakovo tradition, but DNA from the plague victims reveals threads of kinship connecting them—and the plague may have made those threads deadly.
Macleod and his colleagues sequenced the DNA of the plague victims, piecing together how they were related and (through radiocarbon dating) when each member of the family died. That data revealed that the plague seemed to have spread among family members, often killing several at close enough to the same time that siblings often share graves.
“The incidence of detected infections among co-buried kin… would be consistent with the transmission of plague among humans, particularly via pneumonic transmission in the scenario of concurrent deaths,” wrote Macleod and his colleagues.
Or as Macleod put it during the press conference, direct spread between people makes a lot more sense than “an outlandish scenario that absolutely everybody got together at the same time and ate the same infected marmot.”
At Ust’-Ida, a young boy shares a grave with his aunt; both had Yersinia pestis in their bloodstreams when they died. The aunt also has a teenage niece buried nearby in a grave alongside a teenage boy who isn’t biologically related to her (it’s hard to tell if they were adopted siblings or cousins, a couple, or just close friends). And the boy’s father is buried nearby in yet another grave.
“It’s so obvious from the way people are buried… that somebody was around to bury the dead that knew who these people were when they were alive,” said Macleod. “And that adds a really really human element to the scientific work that we’ve done, seeing the impact on communities and how these communities responded to this very tragic set of events.”
Nature, 2026 DOI: 10.1038/s41586-026-10540-5 (About DOIs).
HealthNews
1 Sign of Colon Cancer Doctors Say You Shouldn’t Ignore
When it’s caught early, colon cancer is highly treatable. According to Johns Hopkins Medicine, the five-year survival rate of early-stage, localized colon cancer is 90%. One of the best strategies for detecting the disease early is calling your doctor if you experience the number-one sign of colon cancer. Since the illness is often difficult to diagnose, taking action as soon as you notice that something is amiss may be lifesaving.
Meet the experts: John Nathanson, M.D., a gastroenterologist at NewYork-Presbyterian/Columbia University Irving Medical Center; Pratima Dibba, M.D., a gastroenterologist with Medical Offices of Manhattan.
“Colon cancer can be hard to diagnose because it can develop asymptomatically,” explained John Nathanson, M.D., a gastroenterologist at NewYork-Presbyterian/Columbia University Irving Medical Center. “When colon cancer does cause symptoms, they can sometimes be wrongly attributed to other processes like hemorrhoids, infection, or constipation.” What’s more, symptoms may be mild enough that they are disregarded in the early stages of the illness, not turning severe enough to warrant a call to the doctor until the disease has progressed, said Pratima Dibba, M.D., a gastroenterologist with Medical Offices of Manhattan.
So, what signs should you look out for? Dr. Nathanson and Dr. Dibba agreed that the number-one sign of colon cancer for which you should seek treatment is rectal bleeding, or blood in the stool. “Don’t just blame it on hemorrhoids,” said Dr. Dibba. According to the Cleveland Clinic, blood in the toilet after you poop may be coming from anywhere in your gastrointestinal tract, including your colon, which is why it’s crucial to get it checked out to make sure there’s nothing dangerous going on.
In addition to rectal bleeding, the experts we spoke to say that other common symptoms of colon cancer include abnormal or unintentional weight loss, severe abdominal pain, and persistent changes in bowel habits.
Along with watching for the above signs, make sure you’re following your healthcare provider’s recommendations for when and how often to undergo screenings. The Centers for Disease Control and Prevention (CDC) recommends that you begin regular screenings for colorectal cancer after turning 45, though if you are at a higher risk for developing it you may want to begin earlier. Talk to your doctor about the right plan of action for you.
You Might Also Like
HealthNews
Three brothers lost their parents to AIDS. Now they’re on their own : NPR


Whenever it rains, Joseph, Gift and Alumbwe — ages 17, 15 and 12 — scramble to move their clothes to a dry corner of their home, deep in the Copperbelt Province of Zambia. That’s because rain streams through holes in the roof.
“The house is not okay. Even though we live here it’s only because we have nowhere else to go,” says Joseph, speaking in the local language Bemba. “When it starts raining, where we sleep becomes wet.”
For stories about life in our changing world, subscribe to NPR’s Global Health newsletter.
They don’t have to move their mattresses, he explains, because they don’t have any — the boys sold them when they needed money. Instead, they sleep on a bamboo mat on the floor and share a blanket.
Their mother died in January, their father in February. Now these brothers are in the process of figuring out the basics of living alone.
NPR is not using the brothers’ last name because they are minors.
Both parents were HIV positive but had been able to survive because of the daily medications they took to prevent the virus from progressing. When the U.S. overhauled foreign aid at the start of President Trump’s second term, there were major cuts to global health — and disruptions to the U.S.’s flagship efforts to combat HIV/AIDS globally called PEPFAR or the U.S. President’s Emergency Plan for AIDS Relief.
The boys say that, in the overhaul, their parents could no longer get their HIV medications as the program that delivered medication to their remote area suddenly stopped. It took just about a year for both parents to succumb to the virus.
The phenomenon of child-headed households and orphans was a defining element of the early years of the AIDS epidemic in the 1980s and ’90s. But it diminished with major support efforts from the U.S. as well as the widespread availability of HIV medications that dramatically improved life expectancy.
It’s too early for official statistics to capture whether the shifting aid landscape has caused a spike in orphans and child-headed households. However, a reverend in Zambia — Billiance Chondwe — says he’s noticed a change.
NPR profiled Chondwe — affectionately known by his congregation as Pastor Billy — last year as his community dealt with the aid cuts and disruptions. At the time, he told NPR many of his community members had suddenly lost access to their HIV medication as the nearby PEPFAR-funded clinics they depended on had shuttered. Now, he reports, children are paying the price. In his community, he says, parents are dying of HIV. And that’s leading to the return of child-headed households.
He is trying to help 25 newly orphaned children, up from 11 a couple months ago. “There is a lot of stress and pressure,” Pastor Billy says, ticking off a long list of concerns. “They don’t have enough food. Where they are staying [is not suitable]. There’s no support.”
“God can take care of us”
As a teenager, Pastor Billy lost his twin sister to AIDS. “It brought me to my knees,” he remembers. In the decades since then it’s driven him to help others with the virus. Lately, that work has entailed tracking down people whose U.S. funded HIV-clinics closed overnight as a result of aid cuts last year.
Sometimes, he can help people connect with Zambian government clinics to get the medications they need — but not always. Increasingly, he says, he’s finding children scrambling to figure out what to do as their parents get sick without their HIV/AIDS medications. That’s what happened in January when a community member asked him to check on a family living in a remote area. When he got there, he found Joseph and his brothers along with their ailing father.
“There was so much fear in the faces of the boys. There was so much worry and panicking in the face of the father,” Pastor Billy recalls.
Because Joseph’s family lived three, almost four, hours walking distance from the nearest hospital, community health workers — paid for by a U.S. government aid program — had brought HIV medications to their home. U.S. funding cuts changed that.
“In the rural remote areas, there used to be mobile clinics and nowadays it is not there,” says Pastor Billy.
The boys watched as AIDS took hold and their parents grew weak and lost their appetite. Soon they were losing weight rapidly and struggling with diarrhea. They didn’t have the strength to walk to the hospital. So the family came up with a plan of action.
“We started selling things in the house,” Joseph says. “Whoever wanted to buy a mattress, we would sell. Whoever wanted pots, we would sell.”
The money was to pay for a motorcycle taxi to get to the hospital.
Each night the boys would kneel in the dark and pray for help. The final months were fraught and painful as their parents argued about how the virus had been introduced into their household and worried about what would happen as their condition worsened. Their mother ended up going back to her sisters’ place and dying there. Once their father died, Joseph says, he had no idea what to do.
“We started going to church so that God can take care of us,” he says.
“Creating orphans at a remarkably rapid rate”
When the HIV/AIDS epidemic first hit Africa, the virus was infamous for killing people in their child-bearing years — and “creating orphans at a remarkably rapid rate,” says Dr. Eric Goosby, the second director of PEPFAR from 2009 to 2014 and now a professor of medicine at University of California, San Francisco. That’s what he told NPR last year. “The community around [the kids] rejected them because the stigma for HIV was so severe.”
PEPFAR, which was created under President George W. Bush and grew to be a widely celebrated program, was committed to helping these children.
“We created a system of care that took care of almost 6 million kids every year,” Goosby explains. “It’s a largely unsung story for PEPFAR and it’s the only non-traditional medical intervention PEPFAR heavily funded.”
The system found local adults and provided stipends so they could care for the children and keep them in their home community. PEPFAR also paid for education, nutrition and medical care since about a quarter of the orphans and vulnerable children were HIV positive.
Pastor Billy says he saw how these efforts transformed children’s lives and futures. Now, much of that support network has disappeared. “Cutting [aid] this suddenly has taken us backwards to a place and a season of hopelessness. There is no clear direction, especially on how we can help child-headed homes,” he says.
Asked to comment on these assertions and the situation Joseph and his brothers find themselves in, the State Department sent NPR a statement saying that the U.S. is the most generous country with humanitarian assistance. “If there are such tragic cases happening around the world, it’s not because we’re not spending enough money. It’s because the rest of the world is not spending enough money,” the statement said.
The statement also said: “The United States has not cut health funding, including PEPFAR, for Zambia.”
While appropriations from Congress for HIV have not changed, the money is often not being spent. The Trump Administration is in the process of revamping how the U.S. does global health work and it is trying to hammer out new agreements with individual countries, including Zambia. The Foundation for AIDS Research or amfAR found an almost 20% drop in PEPFAR expenditures between 2024 and 2025 in Zambia and the loss of more than 5,000 PEPFAR staff in the country. In the Copperbelt Province in particular, the amfAR country report shows that thousands of HIV-positive people lost access to their HIV medications between 2024 and 2025.
“The children they left behind”
As his family life turned upside down, Joseph says he had no choice but to drop out of school and give up on his dream of becoming a doctor. Unable to pay rent, the boys moved several hours away to the small, dilapidated house with the leaky roof where rent is minimal.
“Sometimes the roofing sheets will start coming off because of the wind,” Joseph says.
Joseph got a job as a part-time security guard so he could provide a home for himself and his brothers — and so they can continue their schooling. As he puts on his uniform for work, his brothers head to school. Gift wants to be an engineer and Alumbwe a soldier. While school is free in Zambia, the boys struggle to pay for school books. But they still attend class.
When Joseph is not at work, he says, he’s either doing odd jobs to make additional money or trying to get medication for his two brothers, who are both HIV positive. Their clinic is still an hours-long walk away with a multi-hour wait once there.
Waiting in those lines, Joseph says, he’s realized how common his situation is. He says he sees many other children in similar circumstances. Sometimes Joseph doesn’t make it to the clinic before they run out of the drugs his brothers need, so they must go a day or so without their pills. Pastor Billy tries to help with the medication pick-up but he too lives far away.
About once a month their Uncle John travels from several hours away to check on the boys.
“It brings me sadness and heartache to see the children [my brother] left behind,” he says in Bemba. He says he feels guilty that he can’t house the boys but his household has not only his own five children but also his late sister’s six children.
Right now, he says, the best he can do is bring food when he visits. “I do some farming and when I harvest those crops I will then share with them,” he says.
“If my parents were still alive”
Joseph says playing soccer was the one reprieve he would get from the weight of his responsibilities.
“I love soccer,” he says.
But right now, he’s not playing.
His sneakers wore through. “If my parents were still alive, I would still be playing. They would have bought me shoes,” he says.
The best he can do now is watch other kids play soccer. He says it makes him happy that at least some kids get to keep being kids.




If Trump's Iran deal is good for the US, why the GOP outrage?
Months of war and a blockade have battered Iran. Its navy is at the bottom of the Persian Gulf. Its...


US lifts naval blockade as Iran supreme leader says Trump made deal 'out of desperation' | BBC News
The US has confirmed it has lifted its naval blockade of Iranian ports, as the Iran deal comes into effect....


Obama's open presidential centre in Chicago. #BBCNews


Canada v Qatar: World Cup 2026 – live
Key events “There’s no point in beating a dead horse,” says Rebekah Voss, gawping at a dead horse, “but I...


NYC celebrates Knicks championship win for first time in over 50 years. #BBCNews


US-Iran deal triggers 60-day period to reach final agreement | BBC News
The US and Iran have signed a 14-point Memorandum of Understanding, triggering a 60-day period to reach a final agreement.


Obama: Some presidential center exhibits reflect 'unfinished business'
At the opening of his presidential center, former President Barack Obama said some exhibits reflect the “unfinished business” of …
From Stevie Wonder to Bruce Springsteen and Christina Aguilera – meet the stars set to perform at Obama Presidential Center opening
The Obama Foundation has unveiled a star-studded list of musical performers for the grand opening of the Obama Presidential Center,...


Who won the US-Iran Deal? | BBC Newscast
Today, the US and Iran have an agreement which extends the ceasefire between the two countries, and is now signed...


Trump approval at all-time lows after Iran war: 'What was the point?'
The US and Iran have signed an initial agreement, kicking off a 60-day period of negotiations on a final deal...
-

 Business5 days ago
Business5 days agoHow much of Musk’s wealth comes from government help? Virtually all of it
-

 LifestyleNews2 weeks ago
LifestyleNews2 weeks ago120 minutes of strength training per week may help extend lifespan
-

 Politics1 week ago
Politics1 week agoWhat to know about the stabbing that set off fiery riots in Northern Ireland
-

 Video6 days ago
Video6 days agoDownload fans say what they love about the festival. #DownloadFestival #BBCNews
-

 Video6 days ago
Video6 days agoWhy SpaceX IPO isn't about space. #SpaceX #ElonMusk #BBCNews
-

 HealthNews7 days ago
HealthNews7 days agoThe people of Okinawa, Japan only eat until they are about 80 percent full, then stop — and the practice has been linked in multiple peer-reviewed studies to lower rates of cardiovascular disease, slo
-

 TravelNews6 days ago
TravelNews6 days agoMy Paternal Instinct Should’ve Warned Me About Netflix’s Maternal Instinct
-

 Food6 days ago
Food6 days agoPope Leo’s plane was grounded. Then the King of Spain stepped in to help